Achondroplasia is a bone growth disorder. Although achondroplasia literally means “without cartilage formation,” the problem is not the forming of cartilage. The problem occurs when the cartilage has difficulty converting to bone, especially in the long bones of the arms and legs.
Achondroplasia is one of a group of disorders called chondrodystrophies or osteochondrodysplasias.
 Achondroplasia may be inherited as an autosomal dominant trait, which means that if a child gets the defective gene from one parent, the child will have the disorder. If one parent has achondroplasia, the infant has a 50% chance of inheriting the disorder. If both parents have the condition, the infant’s chances of being affected increase to 75%.
Achondroplasia may be inherited as an autosomal dominant trait, which means that if a child gets the defective gene from one parent, the child will have the disorder. If one parent has achondroplasia, the infant has a 50% chance of inheriting the disorder. If both parents have the condition, the infant’s chances of being affected increase to 75%.
However, most cases appear as spontaneous mutations. This means that two parents without achondroplasia may give birth to a baby with the condition.
Achondroplasia is a bone disorder affecting about one in every 10,000 infants. It is caused by a mutation in the FGFR3 gene that impairs the growth of bone in the limbs and causes abnormal growth in the spine and skull.
Approximately 20 to 50 percent of all children with achondroplasia will experience a neurological impairment. This is caused by compression created as they literally grow faster than their bones. The stunted bone growth at the base of the skull and the spine can cause the spinal cord and brain stem to become compressed. This can lead to key nervous system structures — like the brain stem, spinal cord, spinal nerve roots and cerebrospinal fluid (CSF) spaces — to also compress. Eventually, this may lead to neurological deficits like:
Cervico-medullary Myelopathy: Compression at the foramen magnum – the bony hole at the base of the skull through which the brainstem and spinal cord exit the skull – can cause a child’s brainstem to “kink.†This can cause a child to have:
- very brisk reflexes
- numbness
- weakness
- difficulty walking
- loss of bowel and bladder control
- sleep apnea – periods during sleep when the child stops breathing.
Brainstem compression can ultimately lead to death if it is left untreated, so parents and physicians of achondroplastic children should watch for the symptoms outlined above.
Hydrocephalus: When the narrowing near the base of the spine prevents cerebrospinal fluid (CSF) from flowing freely around the brainstem or in and out of the skull, the CSF collects in ventricles (spaces in the child’s brain). The resulting condition is hydrocephalus. In babies, the most evident symptom of hydrocephalus is a quickly enlarging head circumference. Additional symptoms include:
- headaches
- irritability
- lethargy
- vomiting

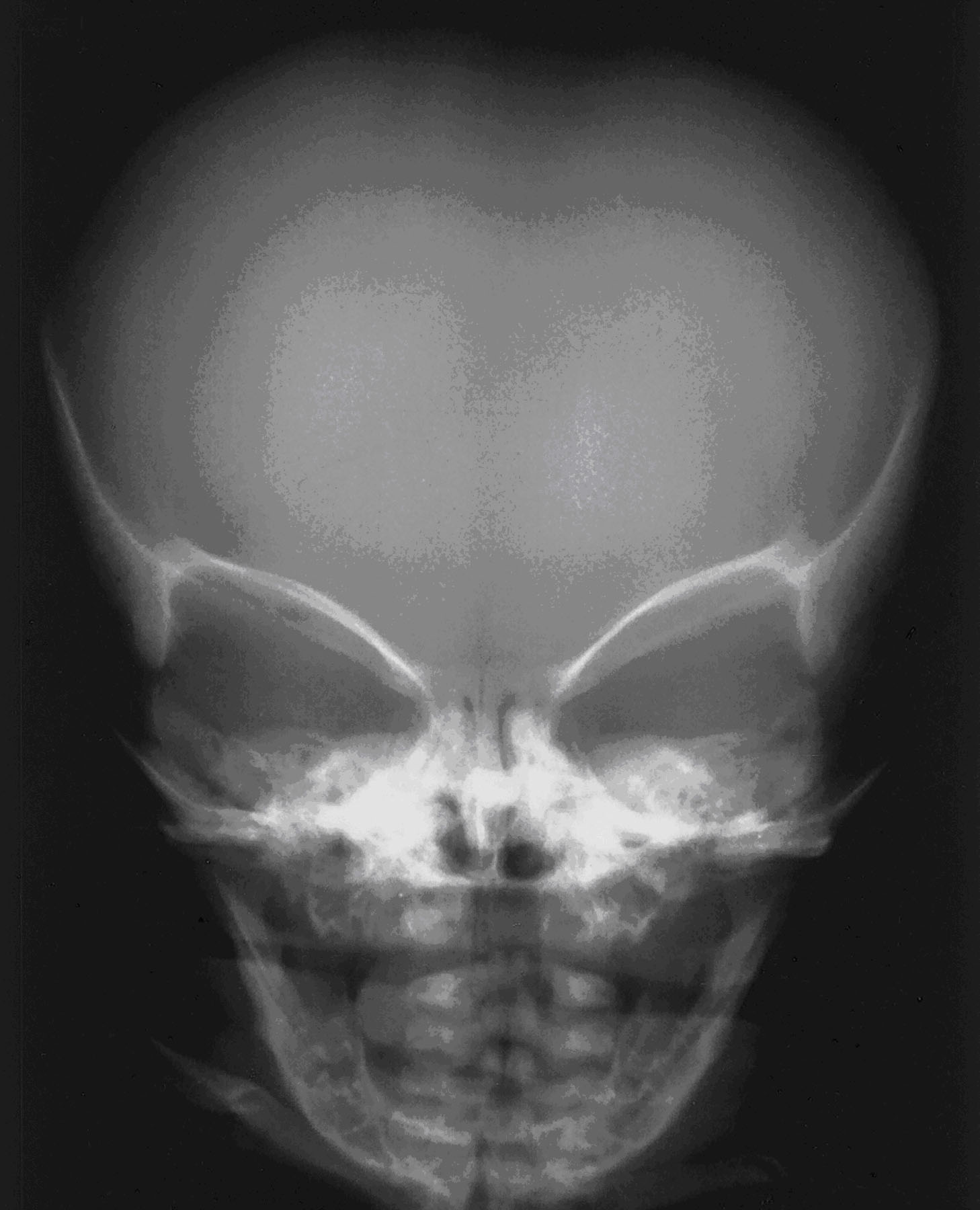
Enlarged head of an individual affected by achondroplasia as seen on x ray
Because an enlarged head is normal in achondroplastic children, pediatricians can use a special head circumference growth chart to distinguish between normal achondroplastic growth and possible hydrocephalus.
Spinal Cord Myelopathy: Sometimes, the vertebrae of achondroplastic children do not grow enough to allow sufficient space for nerves exiting and entering the spinal cord to pass in and out of the bony spinal column. If only a single nerve root is compressed, a child may experience pain, numbness or weakness in a specific arm or leg. They may seem to prefer using one hand over another very early as babies, or complain of pain in their back or affected arm. In more severe cases, the entire spinal cord can be compressed, causing weakness and numbness in the entire body below the spinal cord pinch as well as loss of bowel and bladder control.
Short Stature
All people with achondroplasia have a short stature. The average height of an adult male with achondroplasia is 131 centimeters (52 inches, or 4 feet 4 inches), and the average height of an adult female with achondroplasia is 124 centimeters (49 inches, or 4 feet 1 inch).
Other Symptoms
Other signs and symptoms of achondroplasia can include:
- An average-size trunk.
- An enlarged head (macrocephaly) with a prominent forehead.
- Short fingers. The ring finger and middle finger may diverge, giving the hand a three-pronged (trident) appearance.
- Short arms and legs with particularly short upper arms and thighs.
People with achondroplasia are generally of normal intelligence.
Achondroplasia Symptoms and Health Problems
 Health problems commonly associated with achondroplasia include:
Health problems commonly associated with achondroplasia include:
- Obesity
- Breathing problems (apnea)
- Recurrent ear infections (otitis media).
- Adults with achondroplasia usually develop a pronounced and permanent sway of the lower back (lordosis) and bowed legs. Achondroplasia can also cause back pain in older individuals, which can cause difficulty with walking.
Exams and Tests
During pregnancy, a prenatal ultrasound may show excessive amniotic fluid surrounding the unborn infant.
Examination of the infant after birth shows increased front-to-back head size. There may be signs of hydrocephalus (“water on the brain”).
X-rays of the long bones can reveal achondroplasia in the newborn.
Treatment
There is no specific treatment for achondroplasia. Related abnormalities, including spinal stenosis and spinal cord compression, should be treated when they cause problems.
Outlook (Prognosis)

Comparison between normal child and child affected by achondroplasia
People with achondroplasia seldom reach 5 feet in height. Intelligence is in the normal range. Infants who receives the abnormal gene from both parents do not often live beyond a few months.
Possible Complications
- Clubbed feet
- Fluid buildup in the brain (hydrocephalus)
When to Contact a Medical Professional
If there is a family history of achondroplasia and you plan to have children, you may find it helpful to speak to your health care provider.
Prevention
Genetic counseling may be helpful for prospective parents when one or both have achondroplasia. However, because achondroplasia most often develops spontaneously, prevention is not always possible.