
Acute HIV infection or primary HIV infection (also known as “Acute seroconversion syndrome”) is the second stage of HIV infection. It occurs after the incubation stage, before the latency stage and the potential AIDS succeeding the latency stage.
Symptoms

Rash is one of the symptoms for actue HIV infection
During this period (usually 2–4 weeks post-exposure) an individual may develop influenza or mononucleosis-like symptoms, most commonly fever, lymphadenopathy, pharyngitis, generalized rash of maculopapular type, myalgia, malaise, mouth and esophageal sores, and may also include, but less commonly, headache, nausea and vomiting, enlarged liver/spleen, weight loss, thrush, and neurological symptoms. Infected individuals may experience all, some, or none of these symptoms. The acute illness can last between a few days and 10 weeks, though usually less than 14 days. In some very rare cases, about 10 patients from 1989 to date, a bilateral facial palsy has been associated with acute HIV-1 infection.
Because of the nonspecific nature of these symptoms, they are often not recognized as signs of HIV infection. Even if patients go to their doctors or a hospital, they will often be misdiagnosed as having one of the more common infectious diseases with the same symptoms. Consequently, these primary symptoms are not used to diagnose HIV infection as they do not develop in all cases and because many are caused by other more common diseases. However, recognizing the syndrome can be important because the patient is much more infectious during this period.
These nonspecific symptoms can also be symptoms of other infections; consequently, having these symptoms does not reliably indicate the presence of HIV.
|
History and physical findings for primary HIV infection |
||
|
sensitivity |
specificity |
|
| Fever | 88% | 50% |
| Malaise | 73% | 58% |
| Myalgia | 60% | 74% |
| Rash | 58% | 79% |
| Headache | 55% | 56% |
| Night sweats | 50% | 68% |
| Sore throat | 43% | 51% |
| Lymphadenopathy | 38% | 71% |
| Arthralgia | 28% | 87% |
| Nasal congestion | 18% | 62% |
Cause
Findings of sexually transmitted disease
Primary care physicians will be the first to encounter many of the new cases of HIV infection. Because the source person usually will not have appeared to be ill during contact, the newly presenting symptomatic patient will not recognize the possibility of having acquired HIV infection. However, when a patient presents with fever and fatigue, a sexually transmitted disease or a suggestive symptom complex, the possibility of HIV exposure or high-risk behavior should be reviewed.
Besides obviously risky behavior such as unprotected sex (vaginal, oral or anal) and intravenous illicit drug use (involving shared needles or a common “cooker†into which several syringes are dipped), less obvious sources of HIV infection should be investigated. Young athletes have been known to inject testosterone using a shared syringe. The shared, sharpened plastic “straw†used to sniff cocaine may transmit HIV by way of the nasal mucosa. Body piercing and tattooing may increase the risk of HIV exposure. Occupational exposure is a possible but rare source of HIV infection in health care workers.
Acute HIV infection is a period of rapid viral replication that immediately follows the individual’s exposure to HIV leading to an abundance of virus in the peripheral blood with levels of HIV commonly approaching several million viruses per mL. This response is accompanied by a marked drop in the numbers of circulating CD4+ T cells. This acute viremia is associated in virtually all patients with the activation of CD8+ T cells, which kill HIV-infected cells, and subsequently with antibody production, or seroconversion. The CD8+ T cell response is thought to be important in controlling virus levels, which peak and then decline, as the CD4+ T cell counts rebound to around 800 cells per mL (the normal value is 1200 cells per mL ). A good CD8+ T cell response has been linked to slower disease progression and a better prognosis, though it does not eliminate the virus. A strong immune defense reduces the number of viral particles in the blood stream, marking the end of the acute HIV infection and the start of the infection’s clinical latency stage, which, in turn, may be succeeded by true AIDS.
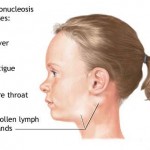
Symptoms of acute HIV are often confused with mononucleosis
The differential diagnosis of the early findings of acute HIV infection can be confusing. Because of a low index of suspicion, the diagnosis is missed in as many as 75 percent of patients. Acute HIV infection may resemble infectious mononucleosis, influenza, severe streptococcal pharyngitis, viral hepatitis, toxoplasmosis or even secondary syphilis. For example, a patient with symptoms suggestive of HIV infection could actually be an HIV-negative young adult manifesting for the first time the effects of a primary immunodeficiency disease involving B-cell and/or T-cell dysfunction. (Immunoglobulin A deficiency—by far the most common immunodeficient condition—often presents after the age of 21 years.) On the other hand, a patient who returns from the tropics with an unexplained febrile illness is frequently assumed to have malaria, typhoid, schistosomiasis, filariasis or an intestinal helminthic infection but may actually have HIV infection. One study found that 3 percent of such travelers were infected with HIV. In areas where AIDS and malaria are endemic, 23 percent of fevers are ultimately attributable to HIV infection and only 15 percent to malaria. Age is also a factor, with the diagnosis of acute HIV infection often delayed in patients over 50 years old.
Differential Diagnosis of Acute HIV Infection
| Primary cytomegalovirus infection |
| Drug reaction |
| Epstein-Barr virus mononucleosis |
| Viral hepatitis |
| Primary herpes simplex virus infection |
| Influenza |
| Severe (streptococcal)Â pharyngitis |
| Secondary syphilis |
| Toxoplasmosis |
| Rubella |
| Brucellosis |
| Malaria |