Treatment
The earlier acute lymphocytic leukemia is detected, the more effective the treatment. The aim is to induce a lasting remission,
defined as the absence of detectable cancer cells in the body (usually less than 5% blast cells on the bone marrow).
Treatment for acute leukemia can include chemotherapy, steroids, radiation therapy, intensive combined treatments
(including bone marrow or stem cell transplants), and growth factors.
Chemotherapy
Chemotherapy for leukemia
Chemotherapy is the initial treatment of choice. Most ALL patients will receive a combination of different treatments. There are
no surgical options, due to the body-wide distribution of the malignant cells. In general, cytotoxic chemotherapy for ALL combines multiple antileukemic drugs in various combinations. Chemotherapy for ALL consists of three phases: remission
induction, intensification, and maintenance therapy.
|
Phase |
Description |
Agents |
| Remission induction | The aim of remission induction is to rapidly kill most tumor cells and get the patient into remission. This is defined as the presence of less than 5% leukemic blasts in the bone marrow, normal blood cells and absence of tumor cells from blood, and absence of other signs and symptoms of the disease. Central nervous system (CNS) prophylaxis should begin during this phase of treatment and continue during the consolidation/intensification period. The rationale is based on the presence of CNS involvement in 10%-40% of adult patients at diagnosis. | Combination of Prednisolone or dexamethasone, vincristine, asparaginase (better tolerance in pediatric patients), and daunorubicin (used in Adult ALL) is used to induce remission. |
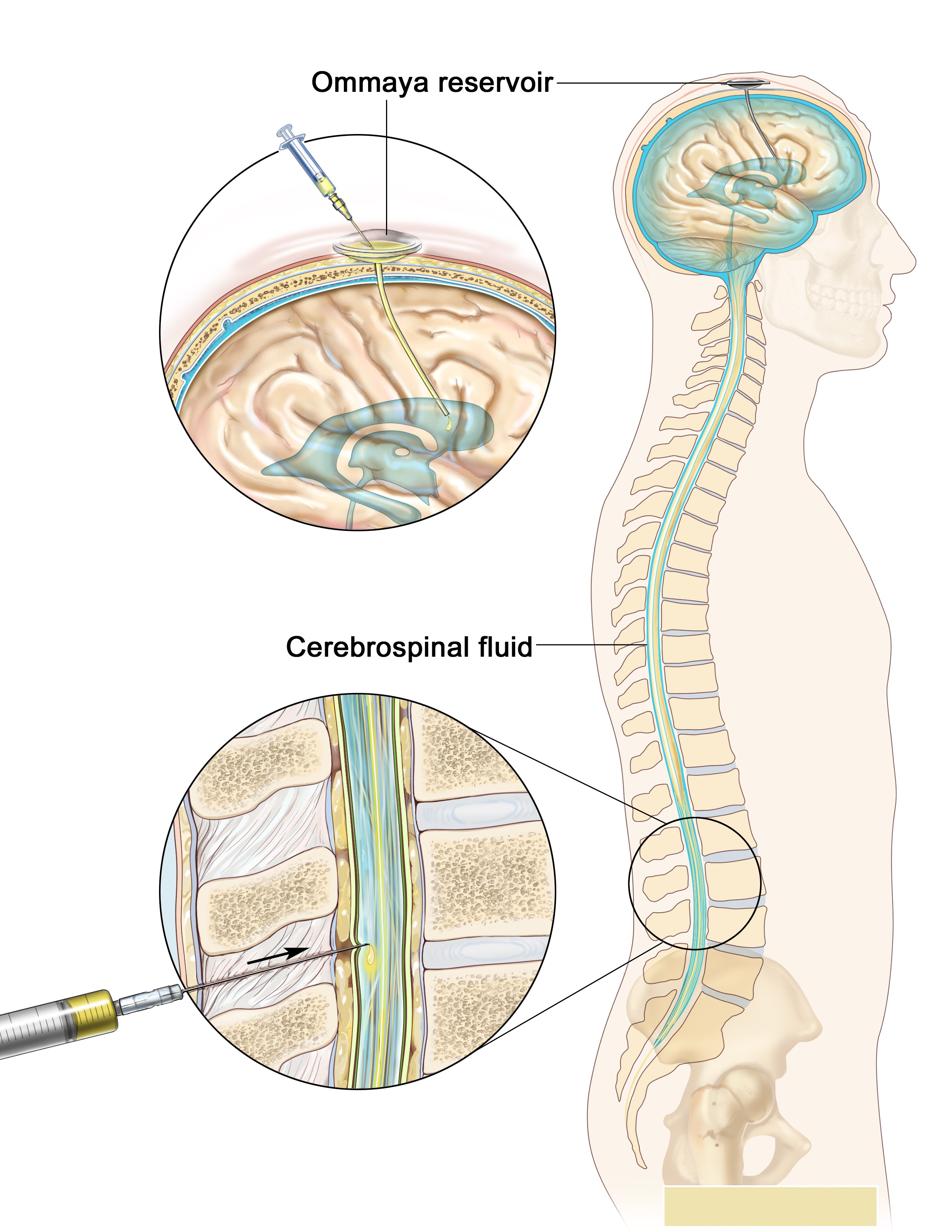
| Consolidation/Intensification | Intensification uses high doses of intravenous multidrug chemotherapy to further reduce tumor burden. Since all cells sometimes penetrate the CNS, most protocols include delivery of chemotherapy into the CNS fluid (termed intrathecal chemotherapy). Some centers deliver the drug through Ommaya reservoir (a device surgically placed under the scalp and used to deliver drugs to the CNS fluid and to extract CNS fluid for various tests). Other centers would perform multiple lumbar punctures as needed for testing and treatment delivery. |
Typical intensification protocols use vincristine, cyclophosphamide, cytarabine, daunorubicin, etoposide, thioguanine or mercaptopurine given as blocks in different combinations. For CNS protection, intrathecal methotrexate or cytarabine is usually used combined with or without cranio-spinal irradiation (the use of radiation therapy to the head and spine). Central nervous system relapse is treated with intrathecal administration of hydrocortisone, methotrexate, and cytarabine. |
| Maintenance therapy | The aim of maintenance therapy is to kill any residual cell that was not killed by remission induction, and intensification regimens. Although such cells are few, they will cause relapse if not eradicated. | For this purpose, daily oral mercaptopurine, once weekly oral methotrexate, once monthly 5-day course of intravenous vincristine and oral corticosteroids are usually used. The length of maintenance therapy is 3 years for boys, 2 years for girls and adults. |
Action of chemotherapy against leukemia
As the chemotherapy regimens can be intensive and protracted (often about 2 years in case of the GMALL UKALL, HyperCVAD or CALGB protocols; for ALL about 3 years, 2 months for males on COG protocols; 2 years, 2 months for females- longer for males as testicles are a potential reservoir), many patients have an intravenous catheter inserted into a large vein (termed a central venous catheter or a Hickman line), or a Portacath, a cone-shaped port with a silicone nose that is surgically planted under the skin, usually near the collar bone, and the most effective product available, due to low infection risks and the long-term viability of a portacath.
Radiation therapy

Down syndrome children have higher chances of being affected by ALL
Radiation therapy (or radiotherapy) is used on painful bony areas, in high disease burdens, or as part of the preparations for a bone marrow transplant (total body irradiation). Radiation in the form of whole brain radiation is also used for central nervous system prophylaxis, to prevent recurrence of leukemia in the brain. Whole brain prophylaxis radiation used to be a common method in treatment of children’s ALL. Recent studies showed that CNS chemotherapy provided results as favorable but with less developmental side effects. As a result, the use of whole brain radiation has been more limited. Most specialists in adult leukemia have abandoned the use of radiation therapy for CNS prophylaxis, instead using intrathecal chemotherapy.
Epidemiology
In the US, the incidence of ALL is roughly 6000 new cases per year (as of 2009), or approximately 1 in 50,000. ALL accounts for approximately 70 percent of all childhood leukemia cases (ages 0 to 19 years), making it the most common type of childhood cancer. It has a peak incident rate of 2–5 years old, decreasing in incidence with increasing age before increasing again at around 50 years old. ALL is slightly more common in males than females. There is an increased incidence in people with Down Syndrome, Fanconi anemia, Bloom syndrome, Ataxia telangiectasia, X-linked agammaglobulinemia and Severe combined immunodeficiency.