
Reveal© device
When it is difficult to assess or record a symptom because it only happens infrequently – as with blackouts – a Reveal© device can be used. The device, which is the size of a packet of chewing gum, is placed under the skin at the left shoulder. You will need to go into hospital as a day case to have this done. A small cut about 2 cm long (just under one inch) is made and the device is inserted. The device monitors the heart’s rhythm and can record any abnormal events that it is programmed to detect. If anything happens, a small box with a button can also be placed on the surface of the skin over the Reveal© device. The device may then be activated by pressing the button, causing it to record the preceding 15 minutes of the heart’s activity. The device can then be ‘interrogated’ by a computer at the hospital and the doctor can examine the recording. The device has a battery that can last up to two years if necessary.
Provocation tests (Ajmaline, flecainide and adenosine tests)

Injection of ajmaline
You may be asked to have this test if your doctor suspects Brugada Syndrome. While you are having an ECG test you will be given an injection of ajmaline or flecainide (antiarrhythmic drugs). The test may show changes on the ECG that are typical of one of the channelopathies.
A fine plastic tube is inserted into a vein at the front of your elbow. The drug is injected over a short period of time (5-10 minutes) and you will be monitored for 20 minutes or a few hours afterwards, depending on the drug used. There is, however, a risk in 1 in 200 Brugada Syndrome carriers or their immediate blood relatives of causing a potentially life-threatening arrhythmia during the injection. The test is therefore always performed with appropriate facilities to protect patients from this risk. Ajmaline is preferable as it lasts a shorter period of time in the circulation.
Adenosine (another short-acting chemical) is given under the same circumstances if Wolff-Parkinson-White Syndrome (WPW) is considered a possible diagnosis.
Cardiac Magnetic Resonance (CMR) scan *
This is a special kind of scan used to examine the structure of the heart and the nature of its muscle. It uses a Magnetic Resonance scanner that creates intense fluctuating magnetic fields around your body while you are inside the scanner. This generates the signals that make up the pictures produced. It may be useful for detecting the presence of fat and scarring in the heart muscle that is associated with ARVC.
Other tests
Coronary angiography and electrophysiological study (EPS)
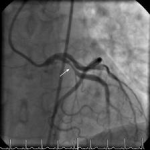
Coronary angiography view
Depending on the results of the above tests, your doctor may suggest that you have other tests such as coronary angiography or an electrophysiological study (EPS). Both these tests are performed in an X-ray laboratory that allows the body and any medical tools (such as cardiac catheter tubes or pacing wires) to be seen using an X-ray camera. You will be asked to lie down on a special moving table and will be given a local anaesthetic in your groin. The doctor will then place fine tubes, called cardiac catheters or electrodes, into blood vessels in your groin. These are gently passed through to the heart. During coronary angiography the coronary arteries (the arteries that supply blood to the heart muscle) are injected with a dye to reveal any furring or blockages – coronary artery disease. (The ECG changes that are characteristic of Brugada Syndrome or LQTS can sometimes be caused by coronary artery disease.)
An EPS (electrophysiological study) involves placing electrical leads inside the heart to analyse its electrical properties and induce arrhythmias. It may be useful in diagnosing Wolff-Parkinson-White Syndrome (WPW) and PCCD and deciding on what treatment to give people with Brugada Syndrome. If the extra pathway seen in WPW is detected at EPS it can be treated there and then by ‘burning’ it away using high frequency radio waves. This procedure is called ‘RF ablation’. There are other tests that may be used to provoke ECG features in LQTS such as ‘cold pressor tests’. A stimulus such as placing your hands in ice-cold water can bring out the ECG features of the condition. This does not appear to increase significantly the likelihood of making a diagnosis but is still used at some centres.
Tilt-table testing
 Tilt-table testing is used to identify other common conditions that can cause blackouts – such as Vasovagal Syndrome or simple fainting – that tend to particularly affect young women and girls but have a very low risk of causing sudden death. These symptoms are very similar to the symptoms of more rare and potentially life-threatening conditions like the channelopathies, so it is important to discover the cause of the blackouts so that the doctor can give appropriate treatment. While you lie flat on a table, your blood pressure, pulse and ECG are monitored. The table is then tilted to an angle of 60 to 75 degrees and monitoring is continued. If nothing happens, a spray of a substance called GTN is given under your tongue as a stimulus and you will be monitored for another 10-15 minutes. The table will then be returned to the flat position and the leads disconnected. The whole test takes around 45 minutes. If your blood pressure falls at the same time as you suffer your usual symptoms, this means that you have Vasovagal Syndrome or a related condition.
Tilt-table testing is used to identify other common conditions that can cause blackouts – such as Vasovagal Syndrome or simple fainting – that tend to particularly affect young women and girls but have a very low risk of causing sudden death. These symptoms are very similar to the symptoms of more rare and potentially life-threatening conditions like the channelopathies, so it is important to discover the cause of the blackouts so that the doctor can give appropriate treatment. While you lie flat on a table, your blood pressure, pulse and ECG are monitored. The table is then tilted to an angle of 60 to 75 degrees and monitoring is continued. If nothing happens, a spray of a substance called GTN is given under your tongue as a stimulus and you will be monitored for another 10-15 minutes. The table will then be returned to the flat position and the leads disconnected. The whole test takes around 45 minutes. If your blood pressure falls at the same time as you suffer your usual symptoms, this means that you have Vasovagal Syndrome or a related condition.
Genetic testing
 In most of the inherited conditions known to cause SADS, mutations of specific genes have been detected and are thought to cause a specific disease. So in principle, if we could identify these mutations, we would be able to make a diagnosis in any DNA sample including any obtained from SADS victims at their autopsy or from their relatives who have given blood. Unfortunately this cannot be done at the moment because we don’t have complete knowledge of all the genes involved in any condition. For example, 7 in every 10 people known to have LQTS have mutations of known identified genes. Also, many variations in the DNA code are found in a large number of people and do not necessarily cause any disease. Many families with LQTS have mutations specific to them (‘private’ mutations) which can also make it difficult to decide whether it is the mutation that is causing the disease or not. As research progresses, more genes will be identified and there will be better tools to decide whether the impact of a mutation causes a disease.
In most of the inherited conditions known to cause SADS, mutations of specific genes have been detected and are thought to cause a specific disease. So in principle, if we could identify these mutations, we would be able to make a diagnosis in any DNA sample including any obtained from SADS victims at their autopsy or from their relatives who have given blood. Unfortunately this cannot be done at the moment because we don’t have complete knowledge of all the genes involved in any condition. For example, 7 in every 10 people known to have LQTS have mutations of known identified genes. Also, many variations in the DNA code are found in a large number of people and do not necessarily cause any disease. Many families with LQTS have mutations specific to them (‘private’ mutations) which can also make it difficult to decide whether it is the mutation that is causing the disease or not. As research progresses, more genes will be identified and there will be better tools to decide whether the impact of a mutation causes a disease.
* Tests marked with a * are non-invasive.
‘Non-invasive’ means that it does not involve penetrating the skin or body.