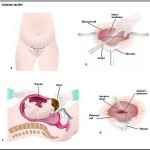
Known as “Endometriosis of the uterusâ€, Adenomyosis is benign and does not cause cancer. Most commonly, the disease affects the back wall (posterior side) of the uterus. The endometrial cells penetrate deep into the uterine muscle (myometrium). When this occurs, the uterus is enlarged usually more than twice the normal size and very hard. The disease may be localized with well-defined borders or diffuse, meaning having no limits or borders. When this localized disease is found it is called adenomyoma. These adenomyomas can be located at different depths of the uterine muscle and can penetrate into the uterine cavity, becoming submucosal tumors.
How common is Adenomyosis?
 This disease can only be diagnosed with 100% certainty by doing a biopsy of the uterine muscle. Depending on the various reported studies published, it has been noted to occur in 8-62% of women who have had hysterectomies. 12% of women with Adenomyosis have also had Endometriosis in other sites such as the pelvic wall, ovaries, fallopian tubes etc. The highest incidence is seen in women in their mid to upper forties, and though this disease may cause infertility, it often appears in women who have already had children.
This disease can only be diagnosed with 100% certainty by doing a biopsy of the uterine muscle. Depending on the various reported studies published, it has been noted to occur in 8-62% of women who have had hysterectomies. 12% of women with Adenomyosis have also had Endometriosis in other sites such as the pelvic wall, ovaries, fallopian tubes etc. The highest incidence is seen in women in their mid to upper forties, and though this disease may cause infertility, it often appears in women who have already had children.
Causes
 The cause of adenomyosis is unknown, although it has been associated with any sort of uterine trauma that may break the barrier between the endometrium and myometrium, such as a caesarean section, tubal ligation, pregnancy termination, and any pregnancy. It can be linked with endometriosis.
The cause of adenomyosis is unknown, although it has been associated with any sort of uterine trauma that may break the barrier between the endometrium and myometrium, such as a caesarean section, tubal ligation, pregnancy termination, and any pregnancy. It can be linked with endometriosis.
Some say that the reason adenomyosis is common in women between the ages of 35 and 50 is because it is between these ages that women have an excess of estrogen (Estrogen Dominance). Near the age of 35, women typically cease to create as much natural progesterone, which counters the effects of estrogen. After the age of 50, due to menopause, women do not create as much estrogen.
Adenomyosis correlates with abnormal amounts of multiple substances, possibly indicating a causative link in its pathogenesis, although correlation does not imply causation:
- Endometrial IL-18 receptor mRNA and the ratio of IL-18 binding protein to IL-18 are significantly increased in adenomyosis patients in comparison to normal people.
- Leukemia inhibitory factor is dysregulated in the endometrium and uterine flushing fluid of women with adenomyosis during the implantation window.
What are the symptoms of Adenomyosis?

Period cramps
As with Endometriosis, patients with Adenomyosis may not show any symptoms (asymptommatic). However, women most commonly experience excessive, heavy or prolonged menstrual bleeding and painful periods (dysmenorrhea). The amount of bleeding and cramps is usually associated with the degree of disease involvement and depth of penetration into the uterine walls. Extensive involvement of the uterine muscle can also interfere with the normal contractility of the muscle which then leads to excessive bleeding.
How is Adenomyosis diagnosed?
An exact diagnosis is often difficult to establish pre-operatively because abnormal patterns of bleeding (dysfunctional bleeding) and fibroid tumors can result in similar symptom patterns. Sometimes during a D&C procedure to remove intra-uterine polyps or small fibroid tumors, tissue is removed enabling a pathologist to make the diagnosis.
·        Pelvic Exam Findings
Pelvic exam findings can reveal a normal, or only slightly enlarged uterus to a very firm tender uterus enlarged to twice the normal size.
·        MRI
At times, this can distinguish adenomyomas from fibroid tumors, but again, experienced physicians and radiologists possessing extensive training are required.
·        Transvaginal Ultrasound
Extensive recent work has been completed with this test, but the amount of false positive results is still high.
·        Tissue Diagnosis
Tissue diagnosis in some form remains the only definitive method for diagnosing Adenomyosis. If the diagnosis is suspected pre-operatively, then a laparoscopy and a long needle biopsy can be performed, whereby a needle is inserted into the back of the uterus to collect a tissue sample for pathological testing. It may also be diagnosed when fibroid tumors are removed.
Can Adenomyosis be treated without surgery?

Progesterone therapy
Some studies have shown that there is a relationship between Adenomyosis and hormone imbalance, most commonly an excess of estrogen. Progesterone therapy, either in the natural or synthetic form has been known to help, but shows very little long term benefits. A medication called Danazol may be helpful in treating the pain and decreasing the size of the uterus but long term positive results are poor.
How can Female Alternative Surgery help Adenomyosis?
Most commonly, hysterectomy has been the mainstay of treatment. Traditional medicine states that since most women with Adenomyosis are beyond child-bearing age, the uterus is no longer relevant. At the Institute, we want to give women every opportunity to retain their female organs even if fertility is not a concern. Our surgical approach is first to make a diagnosis. For women who still wish to conceive, we try to remove the Adenomyosis using laser technology (CO2 Yag and Argon) which preserves the endometrial cavity but treats the remaining deep uterine muscle disease. In the case of women who are not concerned with fertility but want to preserve their organs, our approach is to remove as much of the affected tissue and, if necessary, decrease the size of the endometrial cavity. We treat the remaining uterine muscle with a deep tissue laser technique. Post surgical results have shown that pain almost always disappears and menstrual flow and volume decrease.
Remember: Every form of treatment should be tried before a hysterectomy is ever considered.